TOO LITTLE
ESTROGEN
Anxiety
Bloating
Constant fatigue
Decreased Sex Drive
Depression
Dry
skin
Fatigue that worsens during the day
Headache
Heart palpitaions
Hot flashes
Inability
to reach orgasm
Joint pain, swelling and stiffness
Lethargy & fatigue on light exertion
Low
Back Pain
Memory Loss
Mood swings
Night sweats
Osteoarthritis
Painful intercourse
Rapid
pulse rate
Recent unexplained weight gain
Shortness of breath
Short-term memory failure
Sleep
disorders
Vaginal dryness
Vaginal shrinkage
Yeast infections
|
TOO LITTLE
PROGESTERONE
Anxiety
Asthma
Bloating
Depression
Dry skin
Food Cravings
Fuzzy thinking
Headache
Heart
Palpitations
Hot flashes
Inability to concentrate
Inability to reach orgasm
Insomnia
Irritability
Low
Libido
Memory Loss
Moodiness
Mood swings
Night Sweats
Painful intercourse
Swollen or
Painful breasts
Sleep Disorder
Shortness of breath
Vaginal Dryness
Vaginal shrinkage
Weight gain
Yeast
Infections
|
And then there is Testosterone (also known as Androgen). You say, "but that is a male hormone!". True, but, women's
ovaries and adrenal glands do produce testosterone. Women experience a drop in both estrogen and testosterone production
during menopause. Testosterone is important in maintaining sexual desire, as well as strength and integrity of skin, muscle
and bone. Low levels of testosterone will result in a decreased sex drive, fatigue and decreased sense of well being. For
a further list of symptoms read on.....
TOO MUCH
Acne
Irregular periods
Facial / body hair growth
Thinning of scalp hair
Deepening of voice
Increased
irritability
|
TOO LITTLE
Low libido
Vaginal Dryness
Foggy thinking
Un-associated Aches/Pains
Memory lapses
Incontinence
Depression
Sleep
Disturbances
Bone loss
Decreased muscle mass
Thinning skin |
Now, to muddy the waters just a wee bit more! Following are lists of the symptoms of too much or too little Thyroid Hormone.
We are giving you this to point out the similarities of these symptoms to those of Estrogen and Progersterone.
This is why we tell you to "see your doctor"!
There are three tests that are used to determine the function of your thyroid gland. They are TSH, T3 and
T4. Below the symptom list you can find information about those tests and the results from those tests.
Also here is some information about how the thyroid functions.
TOO LITTLE
THYROID HORMOME
Hypothyroidism
Fatigue
Weakness
Weight gain or increased difficulty losing weight
Coarse, dry hair
Dry, rough pale skin
Hair loss
Cold intolerance
Muscle cramps and frequent muscle aches
Constipation
Depression
Irritability
Memory loss
Abnormal menstrual cycles
Decreased libido
Tingling in the fingers
Loss of equilibrium
Yellow
skin
Goiter
Hoarseness
Decreased concentration
Irregular or heavy menstruation
Infertility or miscarriages
Slowed
heart rate
Myxedema: fluid infiltration of the
causing puffiness (mainly in the face) |
TOO MUCH
THYROID HORMONE
Hyperthyroidism
Palpitations
Heat intolerance
Nervousness, agitation
Irregular or scant menstrual flow
Insomnia
Breathlessness
Increased bowel movements
Fatigue
Fast heart rate
Trembling hands
Weight loss
Muscle weakness
Warm
moist skin
Hair loss
Staring gaze
Excessive sweating
Decreased concentration |
Thyroid function:
The function of the thyroid gland is to take iodine, found in many foods, and convert it into thyroid hormones: thyroxine
(T4) and triiodothyronine (T3). Thyroid cells are the only cells in the body which can absorb iodine. These cells combine
iodine and the amino acid tyrosine to make T3 and T4. The major form of thyroid hormone in the blood is thyroxine (T4). The
ratio of T4 to T3 released in the blood is roughly 20 to 1. Thyroxine is converted to the active T3 (three to four times more
potent than T4) within cells.. These are further processed to produce iodothyronamine (T1a) and thyronamine (T0a). T3 and
T4 are then released into the blood stream and are transported throughout the body where they control metabolism (conversion
of oxygen and calories to energy). Every cell in the body depends upon thyroid hormones for regulation of their metabolism.
The various test that can be done....
TSH
TSH is measured as a screening test for abnormal thyroid function (either hyperthyrodism
or hypothyrodism). It is also measured to monitor treatment of these conditions. The test is also done in infertile females,
to check if thyroid disease is the cause of infertility.
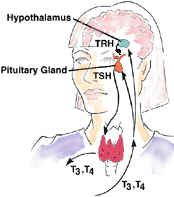
TRH, a hormone produced in the hypothalamus,
stimulates the pituitary gland to release TSH. TSH subsequently stimulates the thyroid to produce thyroid hormones, T3 and
T4. These hormones feedback to the hypothalamus and pituitary to regulate the release of both TSH and TRH.
In certain diseases, this regulation pathway is altered, leading to under- or over-production of thyroid hormone. When a thyroid
disorder is suspected clinically, a TSH level is obtained as an initial test.
T3
T3 is measured as part of a thyroid function evaluation. Most of the thyroid
hormone made in the thyroid is in the form of T4. The body's cells convert the T4 to T3, which is the more active hormone.
Sometimes it can be useful to measure both T4 and T3 when looking at thyroid function. For example, in some cases of hyperthyroidism,
T4 may be normal but T3 will be elevated.
Most of the T4 and T3 in the body is attached to proteins
in the blood. These proteins serve as carriers. The T3 test measures both the T3 that is bound to the proteins and the T3
that is "free" floating in the blood. The free fraction is the hormone that is active.
Conditions that
increase the levels of the carrier proteins -- such as pregnancy and liver disease -- will falsely raise the T3 level. In
these cases, it is useful to measure either the free T3 level or to perform the RT3U test, which gives a measure of the amount
of carrier protein.
T4 and T3 are important hormones in the regulation of metabolism. The exact mechanisms
are not understood, but it is known that T4 increases the concentrations of numerous enzymes involved in the production of
energy in the body.
T4
This test may be performed as part of an evaluation of thyroid function. Thyroid function
is complex and depends on the action of many different hormones:
- Thyroid-stimulating hormone
(TSH) is a secreted by the pituitary gland.
- TSH causes the thyroid gland to produce two more
hormones, T4 (thyroxine) and T3 (triiodothyronine).
- Finally, TSH itself is stimulated by another
hormone, thyroid-releasing hormone (TRH), which is made by the hypothalamus.
In people with normal
thyroid function, having enough T3 and T4 inhibits both TSH and TRH, which prevents the body from making too much T3 and T4.
T4 levels are important, because T4 increases numerous enzymes that produce energy for the body.
Most
T3 and T4 is transported by a protein called TBG (thyroxine binding globulin), but smaller amounts are found on prealbumin
and albumin. When not bound to proteins, they are called "free" T3 or T4.
|
|
|
|
"TSH" Test -- Thyroid Stimulating Hormone / Serum thyrotropin
|
0.4 to 6
0.3 to 3.0 (as of 2003)
|
Under .4 can indicate possible hyperthyroidism. Over 6 is considered indicative of hypothyroidism. Note: the American
Association of Clinical Endocrinologists has revised these guidelines as of early 2003, narrowing the range to .3 to 3.0.
Many labs and practitioners are not, however, aware of these revised guidelines.
|
Total T4 / Serum thyroxine
|
|
Less than 4.5 can be indicative of an underfunctioning thyroid when TSH is also elevated. Over 12.5 can indicate hyperthyroidism.
Low T4 with low TSH can sometimes indicate a pituitary problem.
|
Free T4 / Free Thyroxine - FT4
|
|
Less than 0.7 is considered indicative of possible hypothyroidism.
|
|
T3 / Serum triiodothyronine
|
80 to 220
|
Less than 80 can indicate hypothyroidism
|
Are you ready to learn about one more vital 'hormone' that (in imbalance) can bring on confusingly similar symptoms?
This is INSULIN. While many of us do not have to deal with any form of diabetes we should be aware of the these.
Diabetes is (very simply stated) an imbalance in the insulin our body needs to function properly. If your body is producing
too much insulin your blood sugar levels may drop sharply. If your body is producing too little insulin your blood sugar
levels may rise sharply. Here are the symptoms of both:
Hypoglycemia (low blood sugar) - the result of too much insulin, too little food, or too much exercise.
Symptoms:
Paleness
Trembling
Perspiration
Hot flashes
Cold extremities
A feeling of weakness
Spaciness
Difficulty concentrating
Mood changes
Depression
Difficulty focusing the eye/
blurred vision |
Fatigue
PMS
Rapid heartbeat/palpitations
Hunger/sugar craving
Abdominal pain
Agitation/irritability
Panic attacks
Headaches
Temporary loss of consciousness
Convulsions
Coma | Hyperglycemia
(high blood sugar) - the result of too little, or not enough, insulin or when the body can't use insulin properly.
Type 1 diabetes takes only a few weeks to develop.
The initial symptoms are:
increased production of urine
increased appetite
excessive thirst
fatigue (because the glucose is not being
converted into energy)
loss of weight
feeling sick
dry mouth
dry or itchy skin
poor wound healing (cuts,
scrapes, etc.)
blurred vision
impotence (male)
recurrent infections such as vaginal yeast infections, groin rash,
thrush, or external ear infections (swimmers ear)
If type 1 diabetes is not treated at this stage, the body begins to produce chemicals called ketones that build up in the
blood. This condition – diabetic ketoacidosis – causes additional symptoms:
vomiting
stomach pain
rapid breathing
increased pulse rate
sleepiness
Without treatment, diabetic ketoacidosis can lead to coma or death.
For more information on the connection between Menopause and Diabetes you may want to visit the Women's Health Matters site. For even more information on the relationship between Menopause and Diabetes please read this article from the Mayo Clinic.
First let us touch briefly on a couple of those female hormones and their function. FSH is a hormone that is released by
the pituitary gland in the brain when it senses that estrogen levels are low. This is a normal occurance during the menstrual
cycle.
During a normal menstrual cycle, FSH levels begin to rise slowly a day or two before the your period is due to begin. FSH,
along with the LH (luteinizing hormone), stimulates the ovary to ripen a follicle and release an egg. Then the FSH levels
drops and progesterone levels rise to prepart your uterus for pregnancy or, should the egg not be fertilized, another period.
When the ovaries are slow to respond to the initial release of FSH the pituitary gland releases more FSH in an attempt
to induce the release of an egg. Thus a rise in FSH levels beyond what is normal. This is why high FSH levels may indicate
a perimenopausal or menopausal state during any particular cycle.
When one is in their 30's, 40’s or 50’s the ovaries are more susceptible to external influences
like stress, diet, and external toxins. Cycles may not occur in a perfect textbook manner. You might even have regular
cycles but not release any eggs (an anovulatory cycle).
If your blood or urine was tested during that kind of cycle, your estrogen & progesterone levels might be out of
balance but your FSH level might test normal. You could be having night sweats & hot flashes while still having periods,
then your FSH level might be normal but your estrogen & progesterone levels out of balance. Or perhaps you have skipped
a few periods so your FSH level would be high since your body is trying to stimulate ovulation. In all of these cases
a menopause test kit would indicate that you were menopausal.
Now, lets assume that you start eating better, you begin to take some good supplements, the sun comes out,
and you are more relaxed. Your regular periods could return & your FSH levels drop back to normal. Then a test of
your FSH levels would indicate that you were not in early menopause.
So are we saying you can be both? Yes, you can - because perimenopause is not a set thing. We move into
& out of it depending on our hormonal balance. We can be a little bit menopausal on a now & then basis, actually moving
in & out of it for up to 15 years.
That is why we caution that the menopause tests can be unreliable - because the results are very changeable. They test
for "black or white" conditions and our hormonal balance is gray.
Now - on to those tests...
The most common one is the Follicle Stimulating Hormone (FSH) test. While this test is a good indicator of what your hormone
level is on a given date at a given time it is not a true indicator of where you are in the menopause process. The test most
often run in conjunction with this one is a test for Estradiol. The results of the different tests are interpreted together
to make a diagnosis.
Because hormone levels can (and do) fluctuate, many doctors advise being tested twice - about a month apart. This
is especially important if you are still menstruating or having symptoms. It could be that you are experiencing
what is sometimes known as a "temporary menopause" - a condition that can be brought on by traumatic stress or certain
medications among other things.
Follicle Stimulating Hormone Test (FSH) This test is best done on day
3 of your monthly cycle. If done on any other day it is far less reliable.
The normal range of FSH depends on your age - and various sites list varying numbers.
For women who are menstruating
the normal range is 3 mIU/mL to 30 mIU/mL.
Follicular Phase: 2.5 to 10.2
Midcycle Peak: 3.4 to 33.4
Luteal Phase: 1.5 to 9.1
For women in menopause or after menopause the values range from 30 mIU/mL to 120 mIU/mL.
The Journal Watch, a medical Web site often used by doctors and
patients alike, has this to say about the FSH test:
| |
Is FSH Useful for Identifying Reproductive Stage?
FSH levels vary widely among premenopausal, transitional, and postmenopausal women.
Although follicle-stimulating hormone (FSH) levels are commonly used to distinguish among women in premenopausal, transitional,
and postmenopausal stages, a few small longitudinal studies cast doubt on whether these tests reliably predict reproductive
stages. To examine the usefulness of FSH measurements, investigators used data from 576 healthy women (age range, 35––60;
304 premenopausal, 93 in menopause transition, and 179 postmenopausal) who were examined during the 1999––2000
National Health and Nutrition Examination Survey (NHANES).
Compared with the mean for premenopausal women, mean FSH was threefold higher in women during the menopause transition
(irregular menses during the past 12 months) and sevenfold higher in postmenopausal women (no menses during the past 12 months).
Mean FSH levels were significantly lower in users of postmenopausal hormone therapy than in nonusers. However, considerable
overlap of FSH ranges existed between the menopause-transition and postmenopausal groups, even when hormone-therapy users
were excluded. The optimal cutoff point was 13 mIU/mL (sensitivity, 67%; specificity, 88%) to distinguish premenopausal women
from those in menopause transition and was 45 mIU/mL (sensitivity, 74%; specificity, 71%) to distinguish those in menopause
transition from postmenopausal women.
Comment: These data suggest that FSH has only limited reliability in distinguishing among reproductive stages in women.
What we know is that very high levels of FSH indicate postmenopausal status or absence of ovaries and that mildly elevated
levels suggest that pregnancy might be difficult but not impossible, but no biochemical test accurately distinguishes among
reproductive stages.
—— Robert W. Rebar, MD
|
Estrogen Levels There are three naturally occurring estrogens;
estradiol, estrone, and estriol. These are usually tested at the same time, from the same sample of blood or saliva.
Estradiol: is the primary human estrogen. When your ovaries begin to fail, your circulating estradiol
levels drop. The blood for this test is also drawn on day three of your monthly cycle.
Normal Estradiol day-3 value is 25 to 75 pg/ml
Acceptable ranges:
Female (premenopausal):
20 to 400 pg/mL
Female (postmenopausal): 5 to 25 pg/mL
Usually an estradiol levels about 30 or below when combined with a high FSH level of 30-40 or higher is considered menopausal.
If the estradiol levels are lower than 50 picograms per milliliter, a woman may still be having a period, and may be also
be experiencing symptoms of low estrogen (including hot flashes, vaginal dryness, and sleep difficulties).
Non-menopausal:
Follicular Phase: 24 to 138
Luteal Phase:
19 to 164
Periovulatory: 107 to 402
Postmenopausal:
No HRT: less than 36
With HRT: 18 to 361
Estrone: A standard reference range is not
available for this test. Because reference values are dependent on many factors, including patient age, gender, sample population,
and test method, numeric test results have different meanings in different labs. Your lab report should include the specific
reference range for your test. Lab Tests Online strongly recommends that you discuss your test results with your doctor.
A normal range of estrone in saliva without supplementation for both female and male is 2.6 - 5.4 pg/ml.
In premenopausal women estrone levels generally parallel those of estradiol. After menopause estrone levels increase, possibly
due to increased conversion of androstenedione to estrone.
Estriol: Levels of estriol in non-pregnant women
do not change much after menopause, and levels are not significantly different from levels in men. The time that the most
concern is placed on estriol levels is durning a pregnancy because estriol (along with alpha-fetoprotein, human chorionic
gonadotropin, and inhibin-A tests) is used to assess the risk of carrying a fetus with certain abnormalities, such as Down
syndrome. Estriol is produced by the placenta and thus rises during pregnancy.
Other Ovarian Hormones
Testing these will not indicate if you are definitely menopausal or not, but (depending on your symptoms) you might need
to have one of these homones checked as well.
Testosterone:
Women with low testosterone (yes, women do have testosterone!) may be a problem for a woman with premature ovarian failure
or early menopause (especially women who've undergone surgical menopause).
Total testosterone levels less than 25 ng/dL indicates a deficiency.
Free testosterone levels less
than 1.5 pg/mL indicates a deficiency.
If your levels are only a small amount above these levels, and if you have symptoms such as a lagging libido or excessive
fatigue, it might be advisable to have this hormone checked as you might benefit from some supplementation.
Progesterone:
Menopausal levels are about .03 to .3 ng/ml.
Premenopausal
levels will be about 7 to 38 ng/ml during the luteal phase.
Leutinizing Hormone (LH):
Normal day 3 levels are 5 to 20 mlU/ml.
If your LH levels are high in ratio to your FSH levels, it could indicate that you are not in menopause (or experiencing
premature ovarian failure), but may have polycystic ovarian syndrome (PCOS) which can cause some similar symptoms.
|


